Diagnosis
The reference method for diagnosing rabies is by performing PCR or viral culture on brain samples taken after death. The diagnosis can also be reliably made from skin samples taken before death.[15] Diagnosis can be made from saliva, urine and cerebrospinal fluid samples, but this is not as sensitive. Cerebral inclusion bodies called Negri bodies are 100% diagnostic for rabies infection, but are found in only about 80% of cases.[1] If possible, the animal from which the bite was received should also be examined for rabies.[16]
The differential diagnosis in a case of suspected human rabies may initially include any cause of encephalitis, in particular infection with viruses such as herpesviruses, enteroviruses, and arboviruses such as West Nile virus. The most important viruses to rule out areherpes simplex virus herpes simplex virus type one, varicella-zoster virus, and (less commonly) enteroviruses, including coxsackieviruses, echoviruses,polioviruses, and human enteroviruses 68 to 71.[17] New causes of viral encephalitis are also possible, as was evidenced by the 1999 outbreak in Malaysia of 300 cases of encephalitis with a mortality rate of 40% caused by Nipah virus, a newly recognized paramyxovirus.[18] Likewise, well-known viruses may be introduced into new locales, as is illustrated by the recent outbreak of encephalitis due to West Nile virus in the eastern US.[19]Epidemiologic factors, such as season, geographic location, and the patient's age, travel history, and possible exposure to bites, rodents, and ticks, may help direct the diagnosis. Cheaper rabies diagnosis will become possible for low-income settings: accurate rabies diagnosis can be done at a tenth of the cost of traditional testing using basic light microscopy techniques.[20] REFERENCE:-http://en.wikipedia.org/wiki/Rabies#cite_note-Dacheux2008-14 Diagnosis of rabies in animals
Even with symptoms quite characteristic for rabies, like changes in behaviour or difficulties in swallowing the clinical examination cannot rule out rabies nor confirm the diagnosis. Brain tissue is the preferred specimen for post-mortem diagnosis in both humans and animals.
Intra-vitam diagnosis is in suspect human patients is based on detecting virus or viral RNA in saliva, neck skin biopsy or epithelial cells of the cornea. However, due to intermittent shedding of virus and variable diagnostic sensitivity of the methods applied, only positive results are valid. Detection of rabies antigen
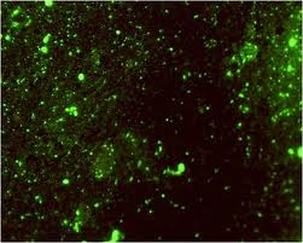
Different immuno-chemical methods have been developed to detect the virus or its antigens. The most widely used method for diagnosing rabies infection in animals and humans and recommended by both WHO and OIE is the fluorescent antibody test (FAT). It is considered the gold standard for rabies diagnosis. Brain tissue samples, smears or cells are treated with antirabies serum or globulin labelled with fluorescein isothiocyanate (FITC). Preferentially polyclonal conjugates with fluorescence-labelled antibodies are used. Specific aggregates of rabies virus antigen are detected by their fluorescence using a reflected light (incident light) fluorescence microscope. The FAT is accurate, sensitive and rapid. Results can often be obtained within 1 to 2 hours of receipt of the specimen.
Recently a rapid immunodiagnostic test (RIDT) was developed. This simple lateral flow test may be used under field conditions and in developing countries with limited diagnostic resources. Detection of rabies virus replication: inoculation tests
The other group of available techniques aim at detecting the replication of the virus on living substrates, e.g. cells or mice. Virus isolation may be necessary to confirm the results of the FAT and for characterization of the virus strain. Virus isolation can be performed on neuroblastoma cells or upon intracranial inoculation of mice
In cells, rabies virus grows generally without cytopathic effect; once again it is necessary to use FAT to confirm the presence of rabies virus in cells. This test is as sensitive as the mouse inoculation test. Cell culture units should be established in laboratories to replace mouse inoculation tests as it avoids the use of life animals, is less expensive and gives more rapid results. In mice rabies induces clinical signs that are relatively typical but it is to confirm with a FAT control. Detection of rabies virus RNA
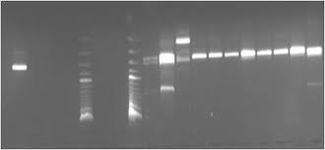
The reverse transcriptase (RT) polymerase chain reaction (PCR) is used to amplify a certain fragment of the virus genome (viral RNA). More recently, real-time PCR has been developed to increase sensitivity and to obtain results even faster. Those techniques have the highest level of sensitivity.
|
Serological tests

Serological assays are not suitable for diagnosis of rabies infections in humans and animals as virus-specific antibodies in serum tend to appear on average 8 days after the onset of clinical symptoms.They are mainly used to evaluate the immune response to human and animal rabies vaccines. The gold standard is the virus neutralisation test. Virus neutralising antibody titres directly correspond to the level of protection. Virus neutralisation assays are also the prescribed tests for international trade and travel with pets. Both FAVN (Fluorescent Antibody Neutralization Test) and RFFIT (Rapid Fluorescent Focus Inhibition Test) are approved for determination of the titre of virus neutralizing antibodies
REFERENCE:-http://www.who-rabies-bulletin.org/about_rabies/Diagnosis.aspx
REFERENCE:-http://www.who-rabies-bulletin.org/about_rabies/Diagnosis.aspx
